
Why IONM in TNTS endoscopic surgery.
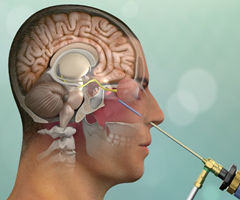
Conventional Skull base approaches TNTS.
- In Neurosurgery the endonasal approach to the anterior skull base was first introduced by Schloffer in1907. The subsequent rapid expansion of endoscopic intracranial surgery has permitted access to large areas of the cranial base and its associated pathology.
- Significant risk to neurological structures if locates in proximity of pathology or a consequence of approach.
- Intraoperative Neurophysiological Monitoring provides for significant reduction in morbidity during these procedures.
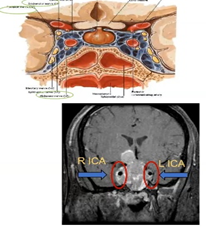
Is pituitary surgery safe , If tumor locating in cavernous Sinus, Transcondylar ,transjugular. chordoma , meningioma and other types of tumors?
- Multimodality Neurophysiological Monitoring provides a real time, comprehensive assessment of Central{CNS} and Peripheral nervous system{PNS} functions.
- And allows for safer and more aggressive management of skull base tumors via the end-nasal route.
Is there any risk factors while approaching ventral skull base via transcribiform, transplanum, transdorsum sellae, transclival, and transpterygopalatine fossa corridors .
- Many reports in the literature have demonstrated the utility of these approaches in reaching the anterior, middle, infratemporal, and posterior fossa.
- Endoscopic endo-nasal surgery { EES} often requires working in close proximity to and occasionally directly on the critical neurovascular structures and cranial nerves that traverse the cranial base.
- Although the reported rates of vascular injury and cranial nerve deficits endo-nasal cranial base surgery are low.
- But complications can have devastating effects, There is a relatively high potential for postoperative morbidity when addressing cranial base pathology.
Intraoperative neurophysiological monitoring {IONM} can be used to further mitigate the risks associated with the Endoscopic Endo-Nasal Approach {EEA}.
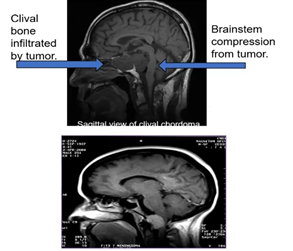
- While approaching above procedure there is possibility of injury Oculomotor nerves , Vascular and also ventral part of the brain stem .
- By the use of intraoperative neurophysiological monitoring can be reduced the morbidity of central and peripheral nervous system .
- Because this multi-modality , physiological test assess the function in real-time during surgery.
What are the modalities to be utilized to monitor major structures? TNTS.
MOTORMEP/CBT MEP TEMG /SEMG .
SENSORYSSEP/BAEP.
- Multimodality IONM has emerged as a standard approach ,to monitoring the nervous system under general anesthesia to improve safety and optimize surgical outcomes across a wide range of surgical procedures involving the central and peripheral nervous system.
- In the terms of the Endoscopic, Endonasal Approach {EEA} to the skull base, multimodal technique somatosensory evoked potentials is likely to be helpful in situations where the internal carotid arteries or their branches are at risk ,In the case of skull base approaches, this includes exposure of the parasellar region and cavernous sinus .
- Similarly, brainstem auditory evoked potentials (BAEPs) are useful for detecting brainstem ischemia during surgery at or around the vertebrobasilar junction, as is the case for transclival approaches .
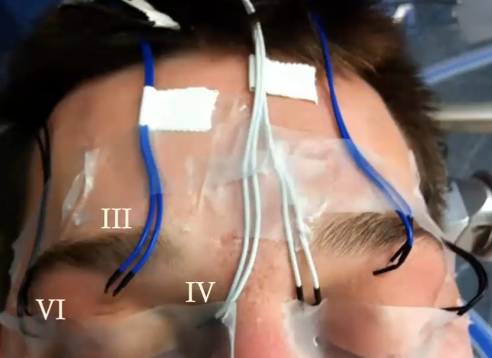
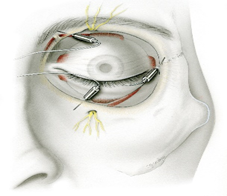
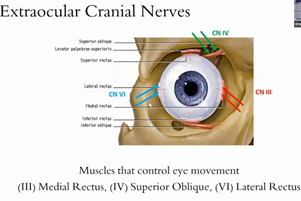
- Intraoperative monitoring of the oculomotor, trochlear, and abducens nerves with needle electrodes placed in the inferior rectus, superior oblique, and lateral rectus muscles, respectively, has long been used during transcranial approaches to the cavernous sinus and is equally applicable in many EEA procedures , including cases in which the cavernous sinus is not accessed.
- Transcranial electrical motor evoked potential monitoring play Important role in case of tumor compressing ventral part of brain stem, means of detecting insult to the long-tract motor pathways. Although detecting functional motor changes.
- Corticobulbar motor evoked potential , Trigger electromyography is also important in case of tumor extending to the lower part of brainstem {Medulla } because this part contains lower cranial nerves {LCNs}.
- Below image showing placement of Recording electrode.


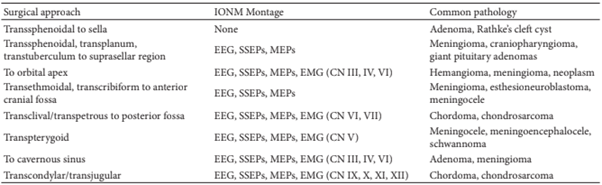
IONM modalities based on pathologies. TNTS.
Stimulation protocol TNTS.
As we using Dynamic / Suction stimulation probe in regularly in cortical and subcortical mapping same this probe can be used in this surgery through EEA instruments for Trigger EMG . Pulse count 1, pulse width 200-300 microsecond @ 2-3 Hz . Intensity of current from 0.5 to 5 milliamp as standard protocol of facial nerve monitoring . for MEP/CBT,MEP C3-C4,C4-C3 Montage is feasible to record both extremities and cranial nerves muscle potentials.
Conclusion. TNTS.
- Neurophysiological Monitoring is standard practice in cranial surgery. In this article we found multi modalities technique is useful to avoid / reduce new neurological problems while approaching Endoscopic endonasal skull base surgery.
- Certainly, not all of these techniques are required for every endoscopic endonasal approach , For example, monitoring is unlikely to be beneficial during the resection of standard pituitary adenomas without cavernous sinus invasion.
Reference .
Fell free to ask Question for TNTS surgery.
- Placement of Electrode ?
- Choice of Anesthesia Drugs?
- Degree of Needle electrode before placement especially oculomotor muscles?
- Can we use regular sub-dermal needle electrode , what we using in regular cases?
- Is really IONM useful in this type of complicated procedure.
This article may be useful for you to understand the concept of ,complicated steps of Intraoperative Neurophysiological Monitoring in TNTS.
Related to this topic.
https://neurointraoperative.com/wp-admin/post.php?post=1451&action=edit
2 thoughts on “Future of Intraoperative Neurophysiological Monitoring IONM in Endoscopic Trans-Nasal Trans-Sphenoid TNTS Approach For Pituitary Adenomas . ”