
Introduction about corticobulbar tract MEPs

- Corticobulbar motor evoked potentials (MEPs) are used to check the integrity of the cranial nerves motor pathways that originate in the cerebral cortex and project to the brainstem nuclei responsible for controlling facial and neck muscles except oculomotor muscles.
stimulation Details.

- Stimulation electrode to the primary motor cortex, specifically the facial representation area, is targeted for stimulation to elicit corticobulbar MEPs.
Type of stimulation .
- Transcranial electrical stimulation (TES) can be used for corticobulbar MEP stimulation, because magnetic transcranial motor potential is not effective in intraoperative due anesthesia affect.
Stimulation threshold .
- The stimulation intensity is set to a level sufficient to trigger MEP responses.
- The stimulation parameters can be used short train.
- consisting of three to five pulses of 500 microsecond pulse duration each. These stimuli may be separated by 2 or 4 ms interstimulus interval { SI}, with a train repetition rate of 2 Hz and an intensity of up to 120 milliampere approx. 120-160 Volt.
Note.
- When applied a single stimulus to the same electrodes at few second after delivering a short train of stimuli Fig 1. The rationale for this kind of stimulation is that only a short train of stimuli can elicit “central” responses activation of the CBT for the cranial nerves generated by the motor cortex or the subcortical part of the CBT in most patients under general anesthesia.
- If a single stimulus elicits a response, this should be considered a “peripheral” response due to the spreading of current distally and activation of the cranial nerve directly rather than through the CBT.
- Another one more technique can be chosen a 90-ms interval between the first train and the beginning of the next single stimulus in order to prevent stimulation of the facial nerve when it became hyperexcitable after the first train of stimuli {“subthreshold hyperexcitability”}
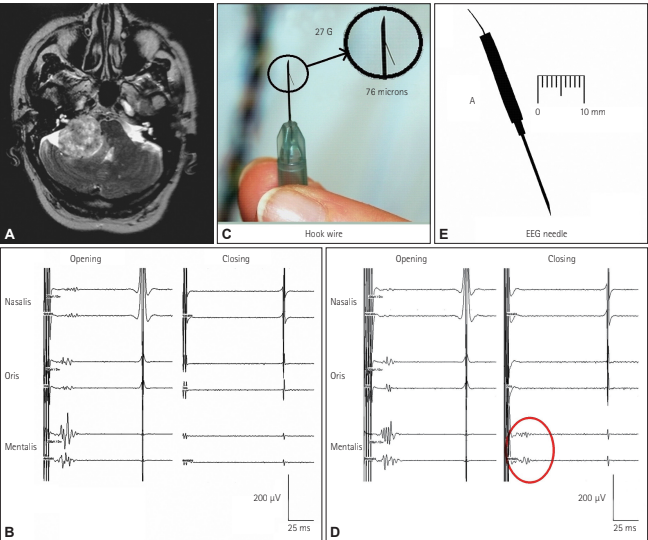
Fig. 1 Corticobulbar MEPs was recorded from the mentalis muscle after Transcranial Electrical Stimulation {TES} of the motor cortex in a patient with a vestibular schwannoma. A. Axial MRI image showing a right vestibular schwannoma. B: Facial CoMEPs recorded with hook-wire electrodes (C) from the mentalis muscle. The facial nerve was accidentally damaged during surgery, after which the facial CoMEPs disappeared (closing). D: Facial CoMEPs recorded with an EEG needle (E) from the mentalis muscle. After damaging the facial nerve there was still a recordable response {red circle}, which was considered to be a far-field response of surrounding muscles such as those of the tongue and other (closing).
Recording Parameters.

- To record the signal subdermal needle electromyography (EMG) electrodes are placed over the target muscles involved in facial movements example orbicularis oris , oculi mentalis and rest of lower cranial nerves innervated myotomes e.g soft palate and trapezius muscles etc.
- Recording Configuration. Differential recording techniques are used to monitor the MEP responses from the target muscles relative to a reference electrode.
Filter settings

- Amplification and Filtering EMG signals are amplified and filtered example bandpass filter settings between 30-1500Hz to enhance the recording quality while reducing noise interference with the help of notch filter.
Conclusion.

Consciously adjusting the stimulation and recording parameters, electrophysiologist can change above given parameter for stimulation and recording to accurately assess the corticobulbar motor pathways and detect any abnormalities that may indicate interruption of motor cranial nerves pathway.
Related to this article.
https://neurointraoperative.com/wp-admin/post.php?post=1363&action=edit
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6123852
Question.
- Why we use train of stimulation to evoke facial MEP?
- How much current you need to stimulate and record the motor signals?.
- Where has to place to recording electrode?.
- Magnetic stimulation can be used rather than TCeMEP in intraoperative?
- Should we place the recording electrode ipsilateral to the surgical side?
Fantastic items from you, man. I’ve take note your stuff
prior to and you’re just extremely fantastic. I actually like what you’ve got right here, really like
what you’re stating and the best way through which you
are saying it. You are making it entertaining and you still take care of to keep it smart.
I can not wait to learn far more from you. That is really a wonderful website.
Also visit my web-site … yt converter
The professionalism at 토닥이 truly impressed me.