
Brief.
- During procedure at the sacral region, neurophysiological monitoring several parameters are typically stimulating and recording to assess the function of nerves and muscles in that area. Multimodality parameters helps to evaluate the integrity and functionality of the sacral nerves and along with critical structures.
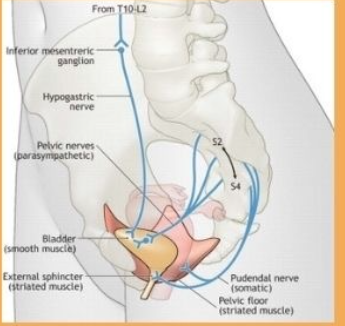
For Motor function at sacral region.
Electromyography Activity
Stimulation.
- Concentric bipolar Electrical stimulator probe will applied to the nerves innervating the floor of pelvic muscles or anal sphincter. Stimulation parameters will be same like what we use in regular cauda equina type of surgery . Intensity of current start from 1.5 milliampere up to the threshold at the rate 2-3 Hz with single pulse , pulse duration 200- 300 microsecond .
Recording .
- Lower-extremity and anorectal EMG activity will be monitored with standard 3 centimeter long subdermal needle electrode from tibialis anterior [TA] as the control recording and external anal sphincter (EAS) or Disposable urethral catheters Electrode, along with L5-S1 innervated myotomes like Extensor Hallucis Longus[EHL] and Abductor Hallucis Brevis [AHB] , L4-S4 nerve roots / plexus.
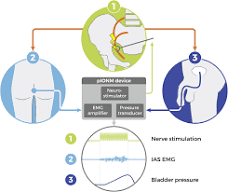
- Image showing stimulation and recording.
Free Run Electromyography at sacral region.
- Above given name of the muscles for Triggered electromyography same channel will be for recording to see the any abnormal activity like mechanical or stretching injury for real time information.
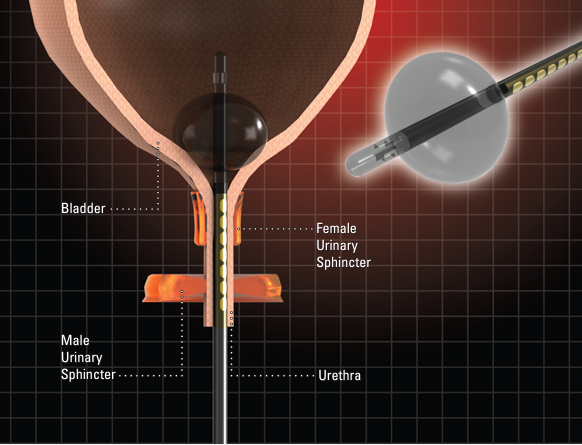
Image of Disposable urethral catheters Electrode.
Transcranial Electrical Motor Evoked Potentials.
Stimulation
- Stimulation can be delivered by transcranial electrical stimulation via corkscrew .
- Electrodes in the scalp at C1/C2 or C3/C4 for monitoring lower extremities .
- A train of 5–7 pulses can be set at 50–75 μs of duration and stimulation intensity at the supramaximal level in a range of 220–380 volts and or set according to threshold .
Recording .
- For control tibialis anterior [TA].
Examination site .
- External anal sphincter (EAS).
- Extensor Hallucis Longus[EHL] .
- Abductor Hallucis Brevis [AHB].
Reflex.
Bulbocavernosus Reflex.
Recording.
- Two bipolar needle electrodes will be inserted on both sides of the external anal sphincter or if other urethral catheter electrode available in your setup, so no necessary to put the EAS electrode, keep secure along with adhesive tape in order to prevent their displacement and outdistanced by rolled sponge.
Stimulation.
- Surface or invasive stimulating electrodes can be used to perform pudendal stimulation. The cathode positioned will be proximal penis or clitoris while the anode on the distal penis or labia majora respectively for male and female. While recording oligosynaptic reflex intraoperatively may be compromised because it is a high susceptibility to general anesthesia mainly for [volatile agents] of Bulbocavernosus Reflex . To avoid these type of challenges TIVA drug will be suitable to record and proper interpretate .
Stimulation.
- Train of pulses at least 3 with 0.3 millisecond pulse duration at rate of of 2-.3 Hz and 15–30 mA intensity of current or as per threshold.
Sensory.
Pudendal Somatosensory Evoked Potentials at sacral region.
- pudendal somatosensory evoked potential [PSSEP] a surface electrode for dorsal of penis or surface/invasive for clitoris .
- corkscrew electrodes can be placed over Cpz [central point at the sagittal midline from nasion to inion] example S1 cortex. and Fz as reference electrode
- The intensity of current will be set up to allow a proper waveform .
Conclusion.
Each of these parameters provides valuable information about the function of the sacral nerves and associated structures, conditions affecting the sacral region, such as pelvic floor dysfunction, fecal and urinary incontinence, and sexual dysfunction.
Questions.
Q-Choice of anesthesia drugs.
A-TIVA-propofol along with remifentanil no relaxant post induction.
Q-Muscle relaxant can be used ?
A- Post intubation should avoid muscle relaxant because TEMG is NMJ response.
Q-Total intravenous anesthesia is suitable to stimulate and record the signals ?.
A-Yes
Q-position of electrode for stimulating and recording?
A-For recording bipolar montage and stimulation concentric bipolar probe.
Q-Reduces incidence of urinary dysfunction ?
A- Yes
Reduction in cases of several sexual dysfunction in women?
A- Yes
Q-Significantly higher mean in international index of erectile function in men?
A-Pelvic floor disorders were reported to be associated with sexual dysfunction including erectile dysfunction male patients.
Q-Higher accuracy in predicting postoperative urinary ,anorectal and sexual function ?
A- Yes with TEMG BCR intraoperative can be prevented from the post operative deficits.
Q-No negative impact on surgery?
A- no.
Related this article.
https://neurointraoperative.com/wp-admin/post.php?post=1942&action=edit
Sir plz provide all modalities electrode placement blog with suitable pictures.👏🏻
Usually i do that but which muscle is requirment particularly.
sphincter muscle
Iliac muscle
And rectus abdominal
If you have plz send me on my mail id Salman.nazeer80@gmail.com
Yes sure Salman i will be sending in your email address.