
Introduction about CP Angle surgery and History.
- In November 1894, Sir Charles Ballance was credited with performing the first successful complete surgical removal of a CPA tumor.
- Intraoperative -Neurophysiological monitoring {IONM} of facial nerve in vestibular schwannoma/meningioma and other type of pathology during cerebellopontine angle (CPA) surgery is crucial for minimizing the risk of facial nerve damage.
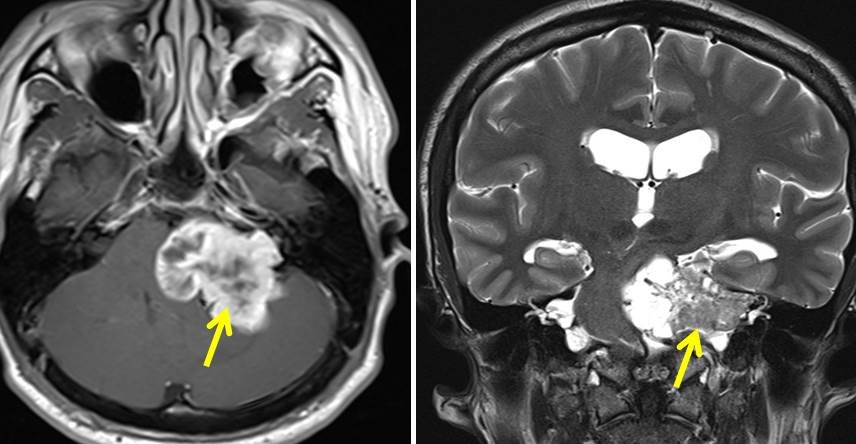
- The CPA is an area in the brain where the cerebellum, pons, and medulla meet, and it’s a common site for tumors like acoustic neuromas or meningiomas.
What are the Preoperative Point/ Preparations. CP Angle Surgery.
- Baseline Assessment/Testing-Before performing Intraoperative -Neurophysiological monitoring IONM Preoperative assessments is mandatory to establish baseline facial nerve function as per House-Brackman Grade I-VI. This includes recording facial nerve responses and motor function tests.
- Electrode Placement- Electrodes should placed to record facial nerve activity on surgical side like if its Right CP Angle surgery which means same side recording to be done because cranial nerve innervates the myotome ipsilateral . These can be either surface electrodes placed on the face or needle electrodes inserted into specific muscles.
House-Brackmann facial nerve grading system I-VI. CP Angle Surgery.

Grade I – Normal–
- Normal facial function in all areas
Grade II – Slight Dysfunction–
- Gross: slight weakness noticeable on close inspection; may have very slight synkinesis.
- At rest: normal symmetry and tone
- Motion: forehead – moderate to good function; eye – complete closure with minimum effort; mouth – slight asymmetry. {Note-Corticobulbar tract supply upper facial bilaterally lower facial unilateral}
Grade III – Moderate Dysfunction
- Gross: obvious but not disfiguring difference between two sides; noticeable but not severe synkinesis, contracture, and/or hemi-facial spasm.
- At rest: normal symmetry and tone
- Motion: forehead – slight to moderate movement; eye – complete closure with effort; mouth – slightly weak with maximum effort.
Grade IV – Moderate Severe Dysfunction–
- Gross: obvious weakness and/or disfiguring asymmetry
- At rest: normal symmetry and tone
- Motion: forehead – none; eye – incomplete closure; mouth – asymmetric with maximum effort.
Grade V – Severe Dysfunction–
- Gross: only barely perceptible motion
- At rest: asymmetry
- Motion: forehead – none; eye – incomplete closure; mouth – slight movement
Grade VI – Total Paralysis–
- No movement
Perioperative Neurophysiological Monitoring. CP Angle Surgery.
- Functional Monitoring of Facial Nerve – During procedure, continuous monitoring of the facial nerve should be done. This is usually done using electromyography (EMG) to record electrical activity from the facial muscles. The goal is to detect any changes in facial nerve function through free run EMG that might indicate potential damage.
- Corticobulbar Tract facial nerve Motor Evoked Potentials– This technique helps to see the function of facial nerve, anatomical continuity as well for gross conduction.
- Stimulation Techniques– The facial nerve will be electrically stimulated to assess its function. The responses are recorded to ensure that the nerve is intact and functioning properly. Both stump proximal to distal .
- Neurophysiological Feedback: Surgeons receive real-time feedback from the monitoring system. This information helps guide the surgical team in avoiding or minimizing damage to the facial nerve.
Postoperative Assessment of facial nerve. CP Angle Surgery.
- Immediate Evaluation: Post-procedure facial nerve function is evaluated to determine if there has been any loss of function. This may involve checking facial symmetry, muscle movement, and other clinical tests.
Benefits point of Monitoring: CP Angle Surgery.
- Enhance Safety: Neurophysiological monitoring allows for real-time detection of nerve damage, enabling immediate corrective actions.
- Improves Outcome: By helping to preserve facial nerve function, monitoring can improve postoperative outcomes and quality of life for patients.

- Intraoperative Neurophysiological monitoring IONM is a specialized and critical aspect of neurosurgery, and it requires a coordinated effort between neurophysiologists, surgeons, and anesthesiologists. The techniques and technologies used can vary depending on the specific requirements of the surgery and the patient’s condition. Role facial nerve MEP No attenuation of the facial MEP indicates no postoperative facial palsy, and severe attenuation of facial MEP mean a possibility of permanent severe facial palsy.
Related to this article.
Intraoperative Neurophysiological Monitoring (IONM) Role in Corticobulbar MEP Transcranial Electrical Motor Evoked potential in skull base and posterior fossa surgery .
https://neurointraoperative.com/p-admin/post.php?post=1363&action=edt
1 thought on “Why Neurophysiological Monitoring in CP Angle surgery?.”