Corticospinal Motor tract monitoring during insular glioma surgery, Deeply Seated Brain Tumors
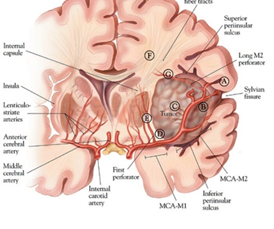
Insular is distinct lobe of the brain , deeply seated brain tumors are located within the cortex .This structure grossly observed deep to the insular operculum which formed by the parietal frontal and temporal lobes. If Glioma involving eloquent areas of the brain , equal consideration should be given to maintain supramaximal extent of resection , to prevent neurological function .
. Intraoperative neurophysiological monitoring is effective and admirable approach .
Surgical approach, Deeply Seated Brain Tumors.
Resection of such a glioma tumor if its involving eloquent areas has an real challenge in surgical treatment to maintain quality of life means patient should walk and talk post surgery.
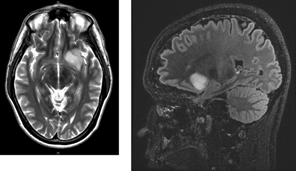
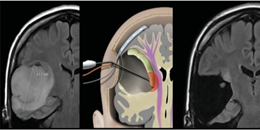
Neuro Navigation with Diffuse Tensor Imaging (DTI)
The role of this imaging technique is virtual to determine the tract , but only lack if brain shifts .
Brain shift during surgery which cause by.
CSF Loss .
Tumor Resection .
Surgical Retraction .
Gravity.
White matter tract shift at 8-15 millimeter (mm) .
Role of Subcortical corticospinal tract Mapping and why is it needed ?
What can be done to prevent motor function while decompressing this type deeply seated Motor Eloquent Brain Tumors.
Removing the last deepest part of tumor near an eloquent area potentially puts neurological function at risk.
Therefore key concept is maximal safe resection.
What can be done .{Deeply Seated Brain Tumors}
.Continuous dynamic mapping with suction probe.
Isolated standard suction stimulator probe ( monopolar) can be use for subpial dissection and simultaneous stimulation at every site and during every step of the tumor excision.
Technique to map the CST.{Deeply Seated Brain Tumors}
Parameters .
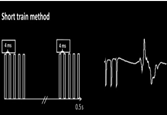
Short train with five biphasic pulses with Inerstimulus interval (ISI) at 2-3 or 3-4 millisecond and 500 microsecond pulse width . Intensity of current can be start from 10-12 milliampere and stop up to 6-5 milliamps , Benefit of especially this train of five pulses parameter does not provoke seizure .
Conclusion.
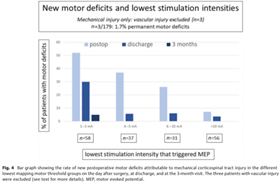
The stimulation intensity of 5 mA indicates the proximity of the probe to the CST by less than 5 millimeters ,means surgeon has to preserve those functional neural structures during dissection of tumor , or otherwise patient can reveal with new neurological motor function deficit.
Feeding artery will be preserve detection of the Vascular injury is not possible with the Subcortical Mapping Technique.
The threshold can be decreased up to 3 milliampere in low grade tumors.
Posterior edge of insular region contains major neural structure which is corticospinal tract means control our motor function, so SSEP
not very important rather than motor.
MEP is not possible these types of cranium surgery because in expose brain difficult to put corkscrew electrode , so direct cortical and subcortical eloquent cortex mapping is useful.



I want to know more about it
YA sure i will send you more details just started my channel this is just beginning but thanks for comment.
Good Information
Thank you
Informative. Thank you for sharing 🙏 excited to know from you
why there is no requirement for MEPs and SSEPs in these types of surgeries?
Posterior edge of insular region contains major neural structure which is corticospinal tract means control our motor function, so SSEP
not very important rather than motor.
MEP is not possible these types of cranium surgery because in expose brain difficult to put corkscrew electrode , so direct cortical and subcortical eloquent cortex mapping is useful.