
Intraoperative Neurophysiological Monitoring of Lower Cranial Nerves.{LCN, i.e. CN IX–XII}.
- Neuro-electrophysiologic monitoring of lower cranial nerves during certain surgeries can be used to provide real time information about potential nerve injury.
- To record the signals, recording electrodes to be placed over muscles innervated by nerves at risk for intraoperative injury.
Name of the muscles innervated by the these nerves.
- LCN IX-Place the subdermal needle electrode on soft palate muscle to record cranial nerve IX electromyography{EMG} .{Note especially for this muscle bend the 3 centimeter long needle electrode at 45 degree because behind or below this myotome passing major vascular structure which is Carotid Artery.
- LCN X-Sensor one endotracheal tube is commercially available while intubation being done a anesthetist them self can put this tube to record recurrent laryngeal nerve EMG -Note–{ make sure the sensor electrode should touch vocalis cord}.
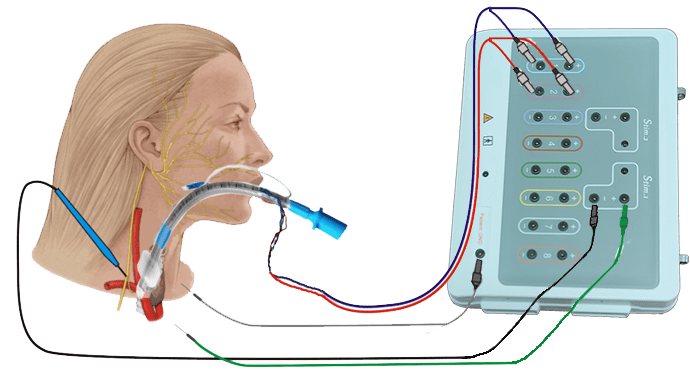
- LCN XI-To record spinal accessory nerve potentials, place the needle electrode over the Trapezius muscle.
- LCN XII-To record Hypoglossal Nerve electromyography put the subdermal needle electrode lateral of tongue.
Principle of neurophysiological monitoring of LCN.
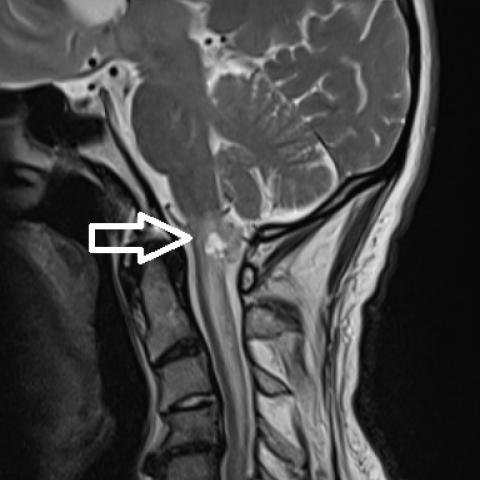
- Medullary tumors, which occur in the brainstem’s medulla oblongata, may affect the lower cranial nerves {IX, X, XI, XII} responsible for vital functions like gag reflex, swallowing, speech, shoulder shrugging and head movement.
Intraoperative Neurophysiological monitoring helps in.
- Assessing Nerve Function-Neuromonitoring provides real-time information on nerve function, helping to identify if a nerve is being compromised by the tumor or surgical intervention/manipulation.
- Preventing Nerve Injury/Damage– It guides surgeons to avoid damaging these critical nerves during tumor resection.
- Evaluating Surgical Outcomes– Post-surgical neurophysiological monitoring helps assess if nerve function is preserved or if there is any deterioration.
Techniques Aspects.
Several neurophysiological monitoring techniques can be applied to monitor lower cranial nerves:
- As a primary modality Electromyography (EMG)– EMG can be used intraoperatively to monitor motor nerve function for lower cranial nerves, EMG helps to localize the nerve nuclei and its motor function of the trapezius (CN XI), genioglossus and other muscles.
- As a secondary modality Free Running EMG– Involves placing electrodes on muscles innervated by the lower cranial nerves to detect any changes in electrical activity.
- Corticobulbar tract motor evoked potential also can be used as a whole tract monitoring like UMN-LMN. And this technique also very much useful to see anatomical continuity and its functions.
- Facial Nerve Monitoring– To assess the function of the facial nerve (CN VII) which is adjacent to other lower cranial nerves
For sensory.
- Brainstem Auditory Evoked Potentials {BAEPs}– These are also relevant for assessing the integrity of auditory pathways, but in some cases, they can provide information about the medullary function indirectly. because eight nerve tract passing from upper medulla .
- Somatosensory Evoked Potentials {SSEPs}– These are also commonly used for lower cranial nerves but may be utilized in cases where sensory pathways are involved.
For motor pathway.
Transcranial electrical motor evoked potentials { TcEMEP}- direct-Indirectly monitoring ventral cord CST fibers while approaching posteriorly for surgical intervention .
Clinical Relevance.
- Preoperative Assessment– Preoperative neurophysiological assessment helps to establish a baseline for nerve function for example if gag reflex is absent one side or both side so here what will be baseline and how and how much will be useful IXth crnial nerve like other also .
- Intraoperative Monitoring– Continuous monitoring during surgery allows for immediate detection of nerve compromise, facilitating timely surgical adjustments.
- Postoperative Follow-Up: Postoperative monitoring helps in evaluating the recovery of nerve function and guiding further rehabilitation if needed.
Challenges.
- Technical Limitations– Accurate placement of electrodes and interpretation of signals can be challenging, especially in complex cases.
- Electrode check-Once electrode placement is done first check impedance to confirm electrode inside of tissue.
- Variability– Patient-specific factors and the location of the tumor can affect the monitoring results and their interpretation.

Intraoperative neurophysiological monitoring IONM is a valuable tool in managing medullary tumors and minimizing the risk of cranial nerve damage, thereby improving surgical outcomes and preserving quality of life for patients.
Related to this article.
https://www.sciencedirect.com/topics/neuroscience/cranial-nerve-monitoring
Nice case! You omitted the LAR (Laryngeal Adductor reflex) intraoperatively – if you are using the ET tube surface electrodes these can be added – as recommended by Tellez, Ulkatan and Mirallave-Pescador -might be worth doing here? and with that lesion the long tracts I would suggest should include SEP as well as MEP to at least arms, as you say MEP more anterior – so the SEP long tracts are more at risk. This not for lower cranial nerves but risk to long tracts with surgery to this lesion. MEPs need to include corticobulbar intraoperatively as you say, with appropriate single shock controls
3cm needles for IX? most don’t use them that long -and still seems to separate from X (which you get if you go lateral to soft palate). The dual prong ones with a plastic hub are easier to insert with Spencer-Wells forceps – and the anaesthetist will usually do it for you! NB re CR X cricothyroid needles are an alternative to ET tube surface electrodes at level of vocalis – gives needle -type high frequency information -these discharges may not be seen as well with surface electrodes, but can’t stimulate with cricothyroid needles so fine for EMG but can’t get LAR reflex.
Note for tongue lateral tongue works as you say – but so does top: and if needles are dislodged can also be inserted during theatre without opeing the mouth, by going up from below the chin, as some prefer for EMG in the neurophysiology lab..
OK? How was the patient post op?
Hello Sir its nice to hear your opinion and i agree with you , i do extremity MEP to see the continuity of CST fibers along with SSEP all limbs , as i mentioned MEP records ventrally and lesion was posterior side of medulla in this case i chose modality MEP-ALL Extremity along with bulbar tract for LCN TEMG {For both LCN along with CST mapping SINGLE pulse for cranial nerve and train of five pulse for corticospinal tract ,SEMG,SSEP.
Conclusion post op- patient did nit develop new neurological deficit along with improvement like slurred speech ,Gag reflex and his left hand was numb also got better .