
Introduction.
Somatosensory evoked potentials [SSEPs] are an excellent modality for spinal cord monitoring during surgery. It covers multiple territory including the
- Peripheral.
- Spinal cord .
- Brain-stem.
- Thalamic .
- Cortical levels of sensory pathway.
- Utility of this modality to monitoring for both spinal cord and cerebral injury during various types of neuro-spine surgery.
- Somatosensory Evoked Potential [SSEP] intraoperative neurophysiological monitoring [IONM] is specific for the dorsal column-medial lemniscus [DCML] pathway but infers protection for other sensory systems as well. Stimulation of mixed peripheral nerves of the upper and/or lower extremity is accompanied by recording from various anatomic generators along the DCML pathway.
Site of stimulation for Somatosensory Evoked Potentials .
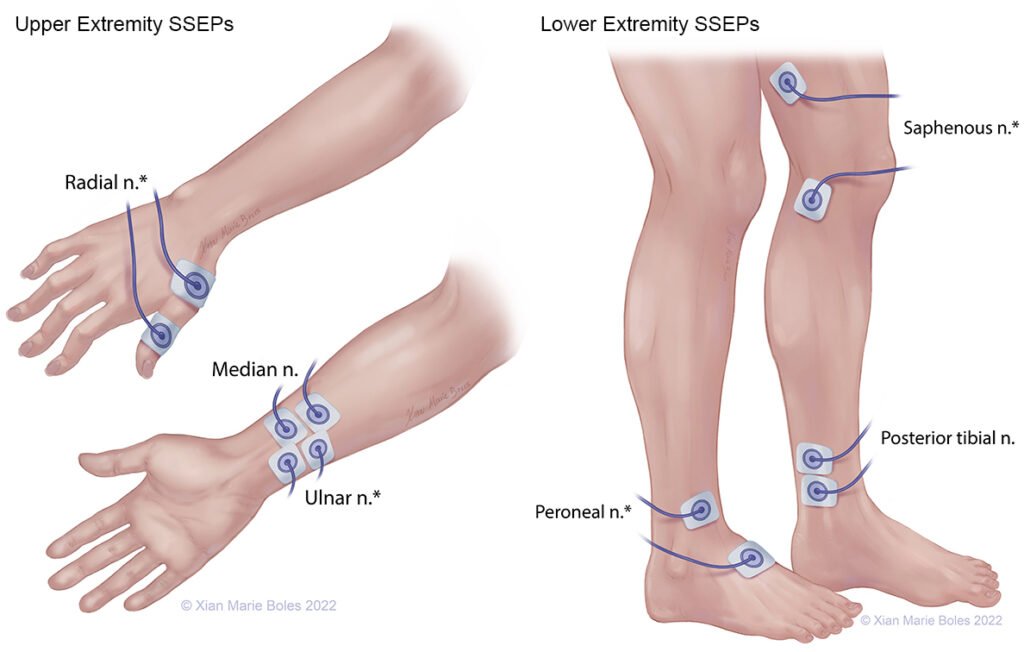
For lower extremity Somatosensory Evoked Potentials
- The posterior tibial nerve (PTN) at the medial malleolus [ankle] is the most common site for lower extremity stimulation. secondary stimulation sites in case of distal neuropathy and amputated.
- For recording several points including peripheral site at either the popliteal fossa or the spine cervical site, and a cortical site (from the scalp).
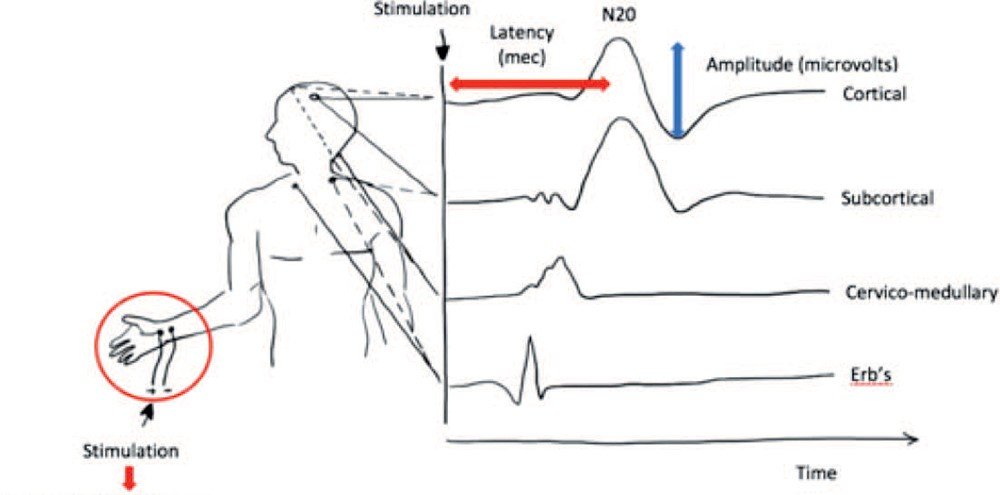
Image of SSEP.

For upper extremity Somatosensory Evoked Potentials.
- Most commonly median and ulnar nerves at wrist [Cubital fossa in case of distally amputated or other ] for stimulation sites . Recording can be done from several points like Erb’s point , cervical and scalp.
Image of stimulating site and along with recording Somatosensory Evoked Potentials.
- The avail of SSEP in IONM is providing an alert to the surgical team of potential neurological complications in real time, resulting in an intervention that will prevent a negative outcome. SSEP may provide the surgeon with reassurance that the surgery is proceeding without complication. This reassurance gives the surgeon the confidence to either complete a procedure or be more aggressive with correction, tumor removal, etc, possibly making the surgery more successful.
Implementation of Somatosensory Evoked Potentials[SSEP].
Role of Somatosensory Evoked Potentials in routine spine procedure.
- Bilateral upper and lower SSEP monitoring is usually used for spine cases. Median, ulnar and Tibial nerves stimulation is included in thoracic and lumbar cases as a means of monitoring for nonsurgical changes such as anesthesia-related changes.
- Ischemia secondary to hemodynamic events can also be detected by SSEP monitoring from all extremities.
Site of stimulation according to spine surgery to rule out pre- post positioning related changes.
- Ulnar nerve monitoring also can help detect an incidental brachial plexus impairment resulting from patient positioning during long surgery. For cervical procedures, median or ulnar nerve pathways are the primary pathways monitored. Because the ulnar nerves enter the spinal cord at a lower level, ulnar nerve monitoring is preferred for cervical cases at and below the C6 spinal level.
- Posterior Tibial Nerve channels can be monitored in cervical cases for detection of a high thoracic or low cervical spinal cord injury. The additional limb coverage also provides greater spinal cord protection from peri surgical events such as hemodynamic changes.
Somatosensory Evoked Potentials SSEP monitoring technique.
Site of stimulation.
- Lower extremity stimulation sites –Posterior tibial nerves at the ankle Or peroneal nerves at the knee, example in patients with peripheral neuropathy
- Upper extremity stimulation sites-Median nerves at the wrist for intracranial cases and cervical cases C5 and above , Ulnar nerves at the wrist for spinal cases at or below C6.
- intensity of Stimulus – Supramaximal [10 % over intensity required to record maximal peripheral response]
- Rate of Stimulus -5.1 per second per nerve, if tolerated with good peaks Or slower if needed to obtain good peaks avoiding harmonics of 50-60.
Recording.
- For upper extremity stimulations Two cortical channels, CPc–CPi and CPc–Fpz.
- A cervical channel- CSp5–Fpz.
- For lower extremity stimulations Two cortical channels, CPi–CPc and CPz–Fpz.
- A cervical channel: CSp5–Fpz.
To identify the Central sulcus [ Pre-central and post central Gyrus].
- SSEPs monitoring also we use for the location of motor cortex.
- The median nerve SSEP stimulation technique is usually used.
- Recording can be done with 6-8 contact strip electrode .
Image of how to identify motor cortex with this test.

Why Somatosensory Evoked Potentials SSEP also useful in cranium surgery.
This modality are useful for monitoring different type of brain cases like brain stem during surgeries to remove
- Cerebellopontine angle tumors.
- Cranial nerve microvascular decompression procedures.
- Brain stem and cerebellar tumor resections.
- Aneurysm clippings or coilings .
- Decompression of Chiari malformations.
- Posterior vertebral artery while working close this artery like C1-C2 fixation and other type procedure .
Clinical indications.
- There are many indications for the use of SSEPs in the operating room.
- The most common use is for spinal cord monitoring in cases involving,
- Scoliosis.
- Cervical myelopathy,
- Fractures.
- Tumors. As well other disorders that put the spinal cord at risk during surgery.
- SEPs also are useful to monitor the intracranial portions of the somatosensory pathways.
Related this article.
https://neurointraoperative.com/wp-admin/post.php?post=2002&action=edit
https://www.ncbi.nlm.nih.gov/books/NBK544358
Question.
Q-Why SSEP is essential in scoliosis corrective surgery?.
A-SSEP is a continues monitoring of cod does hamper the surgical field {to see cord ischemic changes} but MEP we stop the procedure than do because it is high voltage current {jerky movement}.
Q-Is also SSEP prevents brain injury in several cases?.
A-Yes especially in open aneurysm clipping surgery.
Q-Should we avoid OT table plugged in from the power?.
A-Yes
Q-Needle twisted electrode is preferable to stimulate?.
A-Yes but needle should be place at 45 degree means nerve should not get damaged.{ Bar electrode usually missed the location of nerve while turning the patient}.
1 thought on “Somatosensory Evoked Potentials’s utility.”