
Introduction about pedicle screw stimulation.
- Pedicle screws are used in surgeries for the correction of spinal deformity as well as for procedures to decompress neural elements and reduce pain and neurologic symptoms. The function of pedicle screws is to stabilize vertebral bodies following laminectomy and/or discectomy until bony fusion of the adjacent levels is complete.
About pedicle stimulation Test.
- Pedicle stimulation modality in spine surgery is a technique used to confirm the proper placement of pedicle screws within the vertebral pedicles during spinal fusion procedures.
- Trajectory stimulation test involves the use of single pulse electrical stimulation to assess the proximity of the pedicle screw to the nerve roots within the spinal canal. The procedure is typically being performed intraoperatively while the patient position is prone under general anesthesia .
Placement of Screws Accurately.
- Trajectory screws are inserted into the pedicles of the vertebrae using fluoroscopic guidance. The position of the screws is carefully planned based on currently Fluoroscopy, intraoperative computerized tomography (CT) techniques and O’ARM or preoperative imaging studies such as X-rays, BMD, CT scans, or MRI scans.
How to stimulate trajectory before screw.
- Once the trajectory made/pedicle screws are in place, a handheld electrical stimulation monopolar probe is used to deliver low-intensity electrical impulses to the pedicle wall or screw. The probe is placed before placing the screw to [prevent pre-damage of this wall ] or in contact with the screw, and the neuromonitoring team carefully monitors the muscle responses and nerve stimulation thresholds.
Monitoring of Nerve Root .
- Pedicle stimulation is used to detect any inadvertent contact between the trajectory screw and the nearby nerve roots. mal-positioning relies on the fact that bone is an electrical insulator and will limit the amount of current transfer between the stimulated screw and the neural elements.
- A breach in the pedicle wall provides a low resistance conduit of electricity from the electrified screw to the nerve root, which is recordable as a Compound Muscle Action Potential [ CMAP] in the myotome of that nerve root, when the electrical stimulation reaches a nerve root, it will evoke muscle contractions or elicit a pain response in the patient. The surgeon and IONM Team closely observes any responses and adjusts the position of the screw if necessary to avoid nerve injury.
How to confirm accurate placement of pedicle screw.
- By using fluoroscope to anatomical positioning of screw and physiologically a monopolar long stimulation probe, the surgeon can confirm the proper placement of the pedicle screws and ensure that they are placed within the pedicles without impinging on the nerve roots. This helps in real time to reduce the risk of postoperative complications such as nerve damage, weakness or pain.
How to ensure correctly trajectory screw being placed.
- If a large amount of current is required for activation of the nerve roots, it is a reasonable assumption that the bone is intact.
- Lower stimulation thresholds indicate a potential breach. [Note Bone act as a insulator means after some point of current bone will pass the excessive amount of the current to the surrounding nerve root].
- Figure 1 .
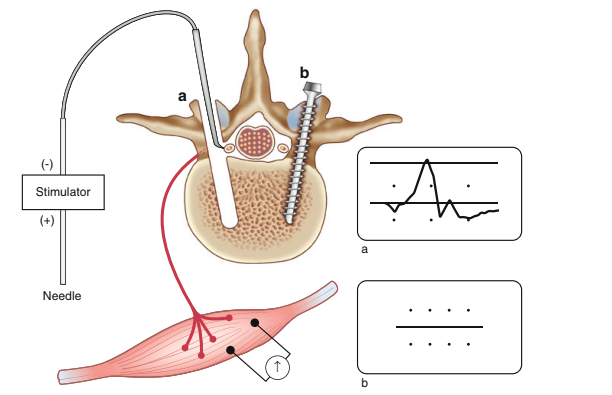
( a ) The stimulation of a screw or hole that is mal-positioned resulting in a pedicle wall breach will pro-
vide a conduit for nerve root activation and a recordable CMAP. ( b ) A pedicle screw or hole that is placed correctly without a breach will not result in a recordable CMAP at moderate stimulation intensities.
Stimulating parameters.
- The stimulation of pedicle screws is commonly performed with a insulated monopolar handheld stimulator with a ball tip. The ball tip is designed to make good contact with the head of the screw.
- A subdermal needle electrode is used for recording signal .
- Square wave pulses of constant current are used having durations of 100–300 μs delivered at a frequency at approximately 2 pulses per second .
- it is imperative that stimulation starts at 4 mA and is advanced in increments of 6–10 mA until a response is seen. A record of the response is made screen capture or save function along with the stimulus threshold, and this is communicated with the surgeon. Stimulation of the pedicle screw provides postoperative evaluation of pedicle screw placement.
- Another commonly used technique is the stimulation of the pilot hole prior to screw placement. Proper stimulation of the hole requires good technique in order to provide an accurate indicator of a pedicle wall breach. Proper technique involves turning the stimulator on and setting the intensity to 8 mA while moving the probe slowly up and down along the pedicular hole. If a CMAP is recorded during stimulation at 8 mA, the intensity should be reduced and the stimulation threshold should be documented.
Interpretation .
- The interpretation of the trajectory screw testing data is not necessarily well agreed upon with some reports advocating an absolute acceptable threshold of 10 mA and other more recent reports, describing the probability of having a misplaced screw when the threshold is in a particular range.
- The recent trend in thinking is that the probability of detecting a medial wall breach increases with decreasing stimulation thresholds. A CMAP recorded at thresholds under 5 mA are highly specific for a breach.
[ Note- Low intensity of current threshold also can show a CAMP response in case of bone quality of patient is poor specially old age or Osteoporosis, microfractures means false positive ] If you get this type of difficulty to interpret the signal first confirm with x, Ray, than IONM team can communicate with operating surgeon, The sensitivity is higher when CMAPs are recordable at stimulation intensities under 3 mA.

- Pedicle stimulation test is a valuable modality in spine surgery for enhancing the safety and accuracy of pedicle screw placement. It provides real-time feedback to the surgeon and helps to minimize the risk of nerve injury during spinal fusion and other procedures.

- Q-How to calculate the threshold of stimulation .?
- A- Usually we go up to 8-10 milliampere if does not elicit any EMG response with this threshold which means its safe {Trajectory}.
- Q-Muscle relaxant drug can increase the threshold of stimulation?
- A- Yes it is increase because this is NMJ response.
- Q-How to confirm the pedicle breach incase of old age bone quality is poor ?
- A-Can be confirmed from the adjacent trajectory.
- Q-How does affect inhalational drugs in this test?
- A- Isoflurane contains some muscle relaxant properties, other like sevoflurane ,desflurane does not act much on MMJ response.
Related this article.
https://neurointraoperative.com/wp-admin/post.php?post=1676&action=edit
would love to always get updated great weblog! .