
Monitoring in Deformity spine scoliosis surgery.
Introduction Deformity spine scoliosis surgery.
The spinal cord damage is one of the most severe complications during thoraco-lumbar pediatrics orthopedic unstable spine surgery . Intraoperative neurophysiological monitoring (IONM) with transcranial electrical motor evoked potentials (TceMEP), somatosensory evoked potentials (SSEP) and Pedicle stimulation test {Trigger electromyogram} (TEMG) ) mitigate the risk of permanent injury and adverse neurological outcomes during the procedure .

Recording
For motor recording place the subdermal needle electrode proximal and distal myotomes lower extremity for surgical site , and also control from upper extremity, to differentiate between true positive and false positive .True positive means signal will change only from surgical site , but in false positive signal will drop globally from upper and lower extremity myotomes , possibilities are physiological reason like hypotension, hypothermia, electrolyte imbalance , bolus dose of anesthesia drugs and other factors like technical glitch.
Interpretation of IONM Signals, Deformity spine scoliosis surgery.
As per Universal methods if signal drops , MEP and SSEP Amplitude > 50-80 percent or all & non. If Latency is shifting 10% OR >10 percent from the base line that means early detection of cord injury , there will be the possibilities of traction, due to iatrogenic injury , ischemic changes , pedicle screw touching {cortical bone trajectory} (CBT) at surgical level .
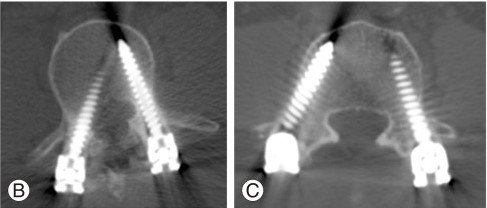
In image showing ‘C’ is normal trajectory but in other image showing trajectory got breach , and according to x ray signal also showing changes.
Choice of Anesthesia Drugs
- Total intravenous (TIVA ) is first preference compare inhalational drugs .
- Propofol , Remifentanil ,Dexmedetomidine , Ketamine .
- Muscle relaxant can be used during surgery but along with antidote Sugammadex
- Reason to Avoid inhalational drugs because its contain some muscle relaxant properties and also more potent .
Conclusions
Intraoperative Neurophysiological Monitoring is useful in scoliosis surgery it is likely to mitigate the risk of new deficits following surgery. Recommend alert criteria for TcMEPs that include multiple facets – amplitude, stimulus paradigm, morphology.
Questions
- Is really IONM helpful in deformity spine scoliosis surgery.?
- Muscle Relaxant can be used during dissection of muscles.?
- Per pedicle screw MEP is required to identified the level of breach ?
- What is mean of fade MEP in long surgery like scoliosis and other as well?.
If find this type {Article} useful. Please share and comment down your suggestions.
Related to this article.
https://neurointraoperative.com/wp-admin/post.php?post=1624&action=edit
2 thoughts on “Is there essential Intraoperative Neurophysiological Monitoring in Deformity spine scoliosis surgery?”