
Aneurysm
How helps SSEP from the stroke post clipping of cerebral aneurysm surgery?.
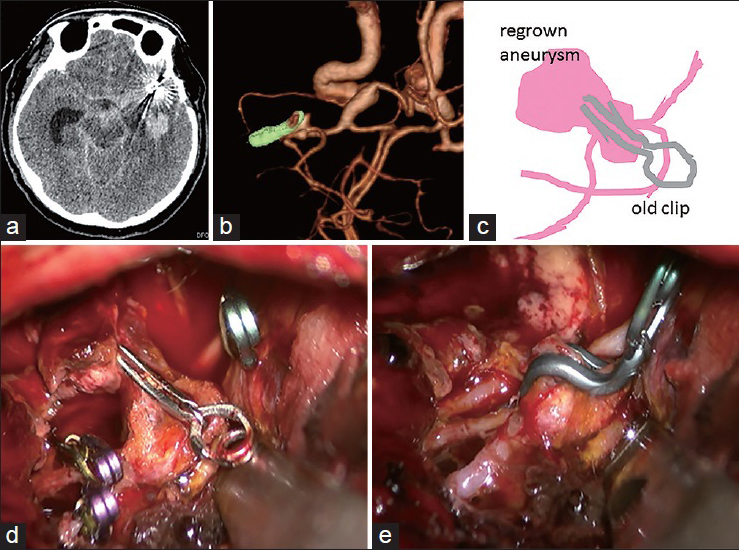
- Cerebral aneurysms are managed via open surgical or endovascular approaches depending on a variety of factors, including the patient’s clinical status and the vascular anatomy.
- Both surgical clipping and endovascular obliteration often are complicated by cerebral infarctions resulting in symptomatic postoperative neurologic deficits.

Intraoperative Neurophysiological Monitoring [IONM] in aneurysm clipping surgery.
- Intraoperative neurophysiologic monitoring (IONM) with the help of somatosensory-evoked potentials [SSEP] usually detect decreases in cerebral blood flow, during procedure allowing the surgeon time for perioperative adjustments that can restore and improve blood flow and result in subsequent reversal of SSEP changes. While stimulating Median nerve and recording from hand area of scalp the latent period usually are N20 millisecond , and stimulating posterior Tibial nerve recording from the leg area of scalp the time delayed around N40-P45 millisecond .
- A prolongation of CCT to more than 10 milliseconds or a reduction in the amplitude of cortical N20,N40 and P45 component of the SSEP by more than 50% is considered significant and a reflection of ongoing intraoperative cerebral ischemia.
- These changes can be corrected, such as removing/manipulating the clip, adjusting the retractor and/or by increasing the blood pressure to prevent the development of clinically relevant postoperative stroke/neurologic deficits.
Changes of signals during on off.
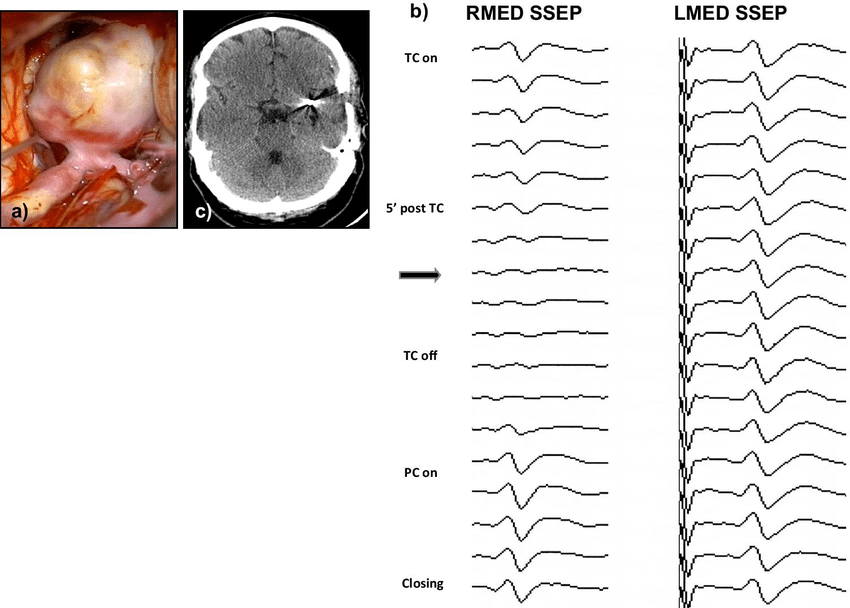
- The time period from arterial occlusion to reversal of SSEP changes to baseline has a direct correlation with development of new stroke/ postoperative deficits.
- Because SSEP amplitude is a reflection of perfusion to the middle cerebral and anterior cerebral artery territories, SSEP monitoring has greater utility when surgical clipping is being performed for anterior circulation aneurysms.
- A correlation between cerebral blood flow and SSEP changes for demonstration, SSEP baseline amplitude is maintained when cerebral blood flow is >16 mL/100 g/min a significant reduction in cortical SSEP amplitude to 50% of baseline is observed when the blood flow is between 12 and 16 mL/100 g/min. studies reveals that when blood flow decreases below 12 mL/100 g/min infarction ensues.
Detecting Ischemia:
- SSEPs detects ischemia or inadequate blood flow to the brain during surgery. Changes in SSEP signals, such as a decrease in amplitude or prolongation of latency, can indicate compromised blood supply to the brain and help alert the surgical team to take prompt action to prevent cerebral ischemia and potential neurological complications.
How SSEPs are Preventing Brain Injury?.
- By continuously monitoring SSEPs throughout the procedure , the surgical team can identify early signs of neural dysfunction or damage and take appropriate measures to protect the brain tissue. Adjusting surgical techniques, modifying anesthesia management, or optimizing hemodynamic parameters based on SSEP feedback can help minimize the risk of brain injury and improve patient outcomes.
Guiding Surgical Decision.
- SSEPs provide objective and quantitative data on the functional integrity of the sensory pathways, which can guide surgical decision-making during Anterior cerebral artery , Anterior communicating artery , middle cerebral artery ,bypass surgery [moyamoya]. Surgeons can use SSEP responses to determine the optimal placement of the transient to permanent clips and bypass graft, assess the impact of vascular manipulations on brain function, and ensure the safe completion of the procedure while preserving neurological function.
Conclusion.
- SSEPs are a informative tool for monitoring cerebral function, detecting ischemia, preventing brain injury, and guiding surgical decision-making Anterior cerebral artery , Anterior communicating artery in middle cerebral artery and bypass surgery. By providing real-time information on the functional status of the brain and central nervous system, SSEPs helps to enhance the safety and effectiveness of the surgical procedure and contribute to improved patient outcomes.
- Perioperative Somatosensory Evoked Potentials [SSEP] monitoring is highly specific for predicting neurologic outcome during and post operative cerebral aneurysm clipping. Patients with postoperative neurologic deficits more likely to have had intraoperative SSEP changes. SSEP monitoring may help design prevention strategies to reduce stroke rates post cerebral aneurysm clipping.
Related article.
https://neurointraoperative.com/wp-admin/post.php?post=1990&action=edit
https://thejns.org/downloadpdf/view/journals/j-neurosurg/137/1/article-p140.pdf
Question.
Q-How helps SSEP in aneurysm clipping?.
A- SSEP useful modality during clipping to see the collateral blood flow, which mans as per signal changes of this potentials intraoperative can be decided to change the location of clipping and also further decision.
Q-How to interpret signal changes of SSEP?.
A-Universal 50% drop signal{amplitude} and 10% latency delayed
Q-Inhalation drugs can be used along with propofol drug?.
A-0.5 MAC is acceptable along with constant TIVA .
Q-Muscle relaxant drug can help to record optimal SSEP?.
A-While recording only SSEP , muscle relaxant is useful because it is act on NMJ and also eliminate motor response.
2 thoughts on “Role of Somatosensory Evoked Potential in cerebral aneurysm to prevent stroke.”