
Brief- Motor Mapping.
- Deeply seated brain tumors represent a special neurosurgical challenge as they are often related to functional eloquent areas of the brain.
- The use of multimodal functional mapping like direct subcortical mapping with monopolar suction probe or monopolar single probe along strip stimulation from the cortical area{Motor strip}.
- Diffusion tensor imaging (DTI) for virtual understanding like approach to chase or decompress the pathology.
- Diffusion tensor and spherical deconvolution tractography can be used to delineate the anatomy of the CST.
- Intraoperative Neurophysiological Monitoring IONM has major role to preserve the functional corticospinal tract fibers while surgeon decompressing the tumors as well as open biopsy of a deeply seated lesion surrounded by the corticospinal tract (CST) using minimally invasive tubular retractors.
In which type of cases Subcortical functional motor mapping can be done to preserve corticospinal tract /internal capsule
Indication of subcortical mapping –
- Insular lesion .
- Caudate nucleus tumors.
- Corona radiata
- Globus pallidus type of pathology or wherever the risk of injury subcortical motor tract .
MRI Scan on of the case.
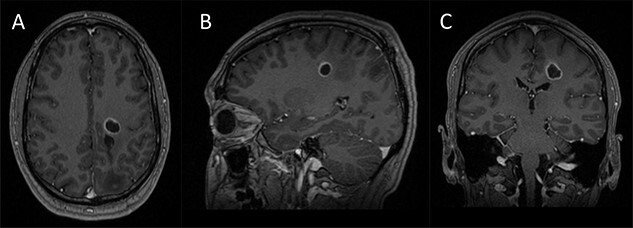
LT Corona radiata lesion.
Another for example.
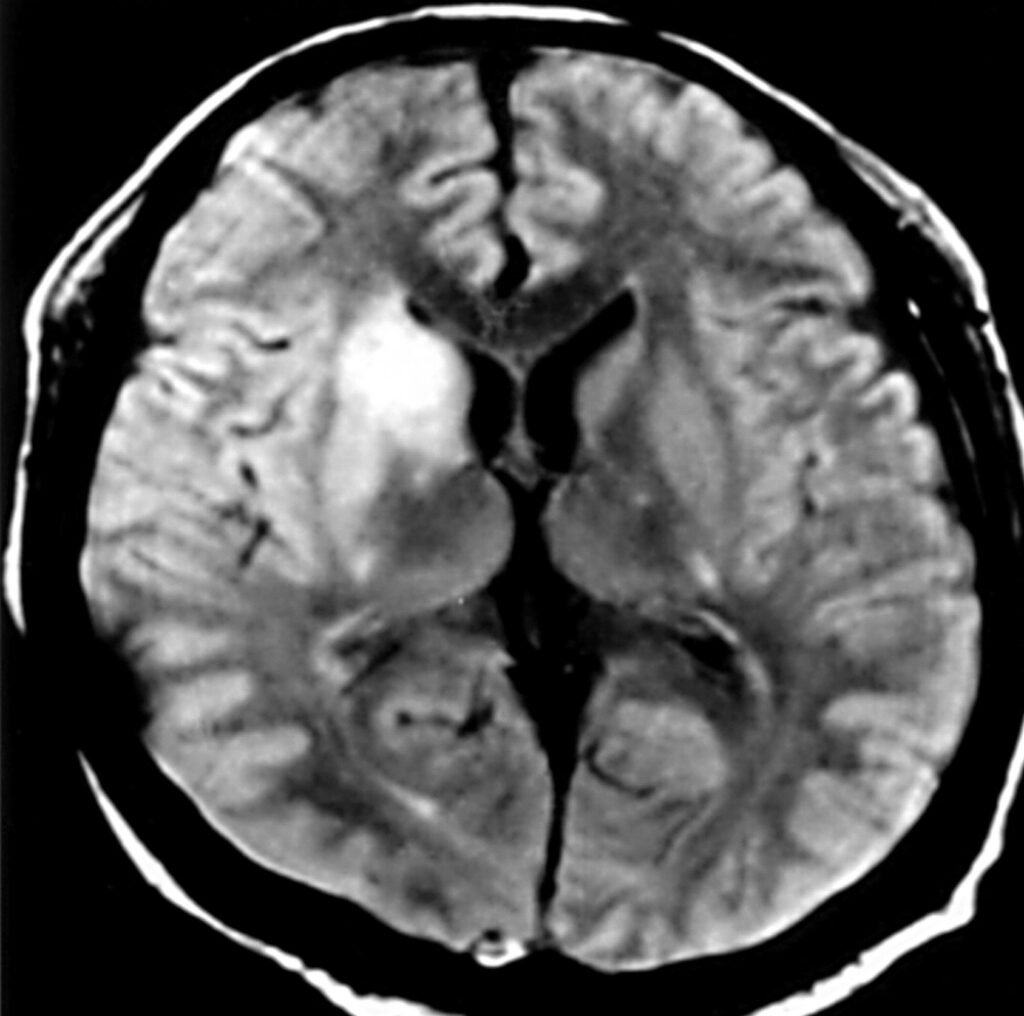
Caudate nucleus tumor.
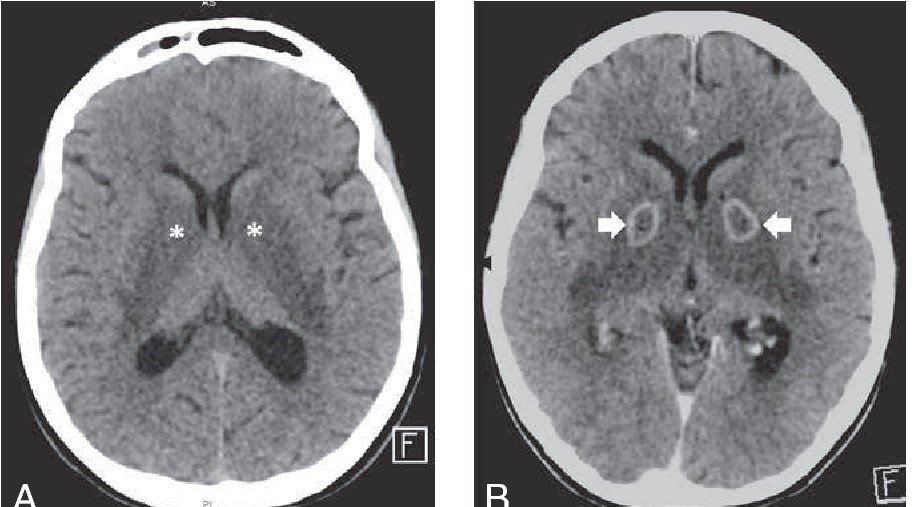
One more example of Globus pallidus pathology.
- Motor mapping is objective modality which means it can be done in General Anesthesia {GA} Or depend on surgeon like awake but while dealing with deep structure pathology awake will be difficult because brain bulging is the major problem. Note-Now a days intraoperative neurophysiological monitoring IONM Mapping technique are very much useful to identify the functional neural structure in real time and surgeon also vey much comfortable with this subject.
Pitfall of mapping.
While motor mapping being done either cortical or subcortical a vascular injury does not prevent mapping technique. {Note – If vascular injury happens during mapping which means immediately does not reflect on signals because ischemic changes to the neural structure takes time and depend on injury , so here false negative possibility will be there.
How to map Corticospinal tract fibers/internal capsule in deeply seated tumors.
- A simple steps we follow either direct monopolar probe or suction monopolar probe .

Why we use only monopolar in subcortical mapping.

- Because calculation of current like one milliampere travels one millimeter which means when we get signals at 5-6 milliampere than we usually stop digging those fibers if surgeon go beyond this limitation so possibility of new neurological motor deficits as per literature . In my practice i follow 5 milliampere cut of in benign tumors like WHO Grade I-II ang i go 6-6.5-7 milliampere in metastasis type of tumor WHO Grade III-IV to maintain quality of life of patient post operative .
Parameters to map and recording the electromyography [EMG] from the muscles .
- A train of five pulses technique are very much useful compere Penfield or ozomen because five pulses technique is easy to record muscle EMG from opposite side of body like tumors on Right side of hemisphere so here recording will be Left side of extremity and neck ,shoulder muscles.
- While stimulation continuous being done with suction monopolar probe so here ice cold irrigation should be used through out the procedure to prevent current deposition related seizure.
Subcortical motor mapping is a modality of intraoperative neurophysiological monitoring IONM subject which preserving cortical–subcortical functional anatomy during surgery minimizing operative morbidity, and maximizing postoperative functional outcomes in patients with deep-seated motor eloquent tumors .This modality is a safe and feasible technique that can be integrated into everyday practice, allowing patients to benefit from a successful functional-sparing approach and a rehabilitation framework for functional recovery after surgery. For further details regarding this subject please read one of my article mapping in insular glioma link given end of topic.
Related to this article.
https://neurointraoperative.com/wp-admin/post.php?post=21&action=edit
QUESTION.
- What is the meaning of Hemi motor evoked potentials in cranium procedure?.
A- Hemi means half which means one side motor evoked potentials either Left OR Right, for example if lesion left side which means MEP will be required Right side of the face to upper and lower extremities as per human homunculus
- Hemi side motor evoked potentials can be done in insular type of lesion?
A-Of course can be done at low intensity of current/voltage
- What is the purpose of Hemi MEP in open brain surgery?.
A-While using cortical subcortical motor mapping one base line should be there to check the integrity of corticospinal tract fibers
- How much voltage is required to stimulate the one side of brain?.
A-Usually 150-200 volts preferable @ 5 pulses ,75 microsecond pule width ,Inter Stimulus Interval 3 millisecond and train rate up to 1 Hz. {Note-power at lest antigravity to apply this modality}.
- How helps this modality to check the function / integrity of corticospinal tract or internal capsule.?
A-Perioperatively some times we do not get confident is there integrity of fibers intact or lost .
- Why our concern about brain bulging when stimulating MEP?
A-Usually avoid especially patient who have history of seizure while doing MEP in this type of case brain bulge is the major problems .{ This type of procedure preferable only cortical and subcortical motor mapping standard train of five pulse technique}.
- How to place corkscrew electrode in cranium cases.
A- Place the electrode little away of incision side for example temporal side craniotomy choose C1-C2 montage if its midline choose C3-C4 or as per possible location to put the corkscrew.
- This modality can be done awake patient?.
A- Of course not because during procedure we check power subjectively.
1 thought on “Subcortical motor mapping in deep structure pathology.”