
Why we should concern to monitored pelvic sacral nerve roots/plexus.
- The floor of pelvic as we know is a complex structure which composed of nerves ,muscles and connective tissues, that support the major organs and contribute to several functions such as urinary and fecal continence, sexual function, and stability of the pelvis. The nerves floor of the pelvic are crucial for coordinating these functions. [These nerves injury during procedure can reveal in bowel either sexual and anorectal dysfunction].
Brief about physiology and anatomy of these structures.
First about Pudendal Nerve.
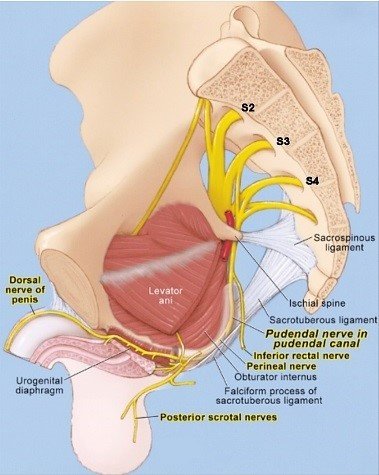
- This is the primary nerve responsible for innervating the floor of pelvic muscles. It comes from the sacral plexus [S2-S4] and travels through the pelvic region, it also supplying sensation to the external genitalia and perineum. The pudendal nerve also plays a significant role in controlling voluntary sphincter muscles involved in urinary and fecal continence.
Second about Splanchnic Nerves.
- These nerves arise from the sacral segments of the spinal cord [S2-S4] and it is contribute to the autonomic nervous system.
- Pelvic nerves Parasympathetic which controls bladder contraction.
- Hypogastric nerve Sympathetic which means bladder relaxation.
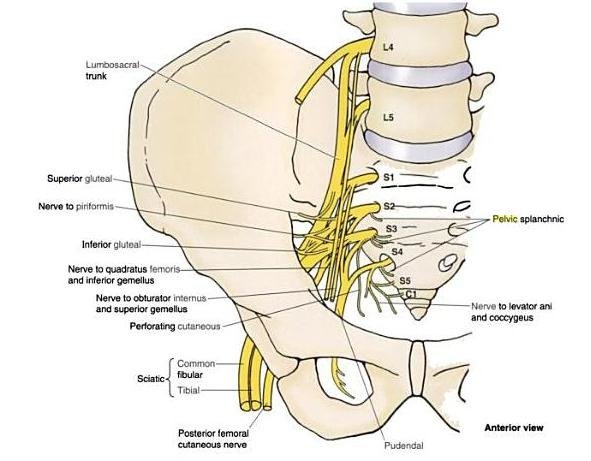
Third Sacral Nerves.
- The sacral nerves, specially S2-S4, give rise to various branches that innervate the floor of pelvic muscles and as well as surrounding structures. These nerves play crucial role in coordinating the voluntary and involuntary muscle contractions necessary for floor pelvic function.
Fourth is Coccygeal Nerve.
- The S5 roots and coccygeal nerves comes from the lower sacral along with coccygeal and this is provide sensory innervation to the coccygeal region. While not directly involved in floor of pelvic muscle function, it contributes to the overall sensory feedback from the pelvic area.
What are the types of procedure puts neurological deficit of the sacral nerves.
Neurosurgery.
- Myelomeningocele
- Tethered cord syndrome
- Cauda Equina tumor and other type of surgery like Sacrectomy ETC.
Orthopedic spine .
- Sacral tumors , lateral spine or others also like where ever the risk of these nerve, Neurophysiological monitoring will be useful to monitor real time information and prevention of neurological deficits .
In General Surgery.
- IONM also plays important role while procedure being done to treat the colorectal tumor.
Uro-surgery.
- Prostate gland .
Gynecology.
- Hysterectomy.
What Intraoperative Neurophysiological does during these type of surgery being done?
Neurophysiological monitoring helps to reduce the risk of sacral nerve damage while procedure being done at floor of pelvic region and also maintain the quality of life from the bladder incontinence, anorectal dysfunction and sexual dysfunction.
What kind of modality to be used .
Multimodal neurophysiological approach will be useful.
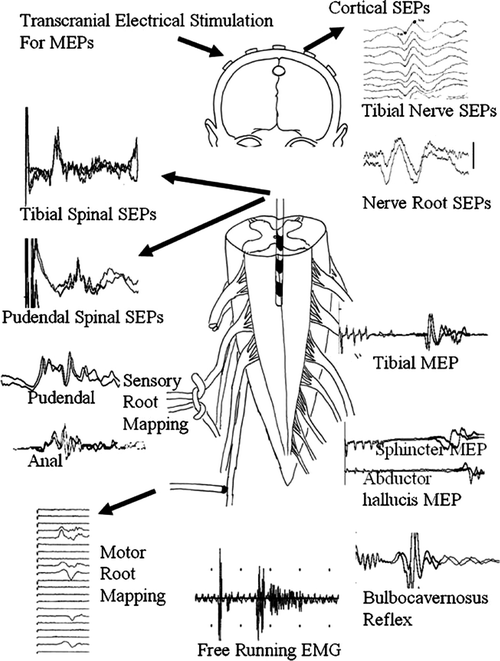
Motor.
- transcranial electrical motor evoked potentials [TcEMEP]
- Triggered-Electromyography [T-EMG].
- Free run Electromyography [F-EMG].
Reflex.
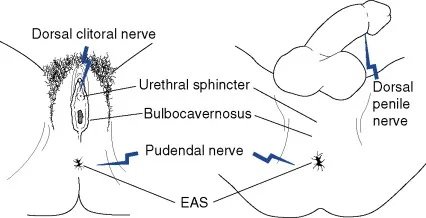
- Bulbocavernosus reflex [BCR].
Sensory.
- Pudendal somatosensory evoked potentials [PSSEP].
- For motor both TCMEP and T-EMG, recording electrode will be same like lower lumber to sacral region.
- Stimulation for Tcmep Head like C1-C2 or C3-C4 , For T-EMG concentric bipolar probe .
- For P-SSEP ,Dorsal nerve penis and clitoris, recording from end of sensory pathways {Post central Gyrus}

For Bulbocavernosus reflex [BCR], reflex of sphincter, sexual function along with polysynaptic reflex.
Benefit of pelvic intraoperative neurophysiological monitoring in Patients With Rectal Cancer.
- Intraoperative Neuromonitoring also prevents dysfunction in Patients With Rectal Cancer, Pelvic floor Intraoperative Neuromonitoring [PFIONM] can also improve urogenital and ano (neo-)rectal functional outcomes in patients who underwent total mesorectal excisions [TMEs] for rectal cancer.
Conclusion.
Intraoperative neurophysiological monitoring {IONM} in floor of pelvic surgery plays a crucial role in ensuring the safety and efficacy of the procedure. By providing real-time information about nerve and muscle function, this monitoring helps surgeon make informed decisions to protect neural structures, minimize complications, and optimize patient outcomes.
Related this article.
https://neurointraoperative.com/wp-admin/post.php?post=1957&action=edit
Question.
Q-What is the major role of Pudendal nerve SSEP in pelvic floor surgery?.
A-Somatosensory evoked potential technique in combination with nerve conduction determination based on neuro-electrophysiologic principle, which can objectively record the conduction time of pudendal nerve in both peripheral and central parts
Q-Why we only choose concentric bipolar probe?.
A-Does not spread much current to other functional neural elements.
Q-Muscle relaxant can affect these type of monitoring?.
A- This is multimodal technique like motor and sensory so NMJ blocker will hamper the signals of motor response.
Q-Inhalation drugs has any role in this surgery?.
A-0.5 MAC acceptable if neurologically intact power {Sevoflurane or Desflurane}-Isoflurane have some muscle relaxant properties.
Great blog! Is your theme custom made or did you download it from somewhere? A design like yours with a few simple adjustements would really make my blog jump out. Please let me know where you got your theme. Many thanks
Its all my text book and my experience. Thank you to read my blog.